The Short Answer: Most supplement interactions aren’t emergencies — but a few can seriously reduce how well your medication works or increase side effect risk. The biggest culprits? Calcium and thyroid meds, magnesium and antibiotics, fish oil and blood thinners, St. John’s Wort with… almost everything, red yeast rice (hidden statin), and one silent killer: potassium supplements with ACE inhibitors.
- Timing fixes most problems: Spacing supplements 2-4 hours from certain meds often solves the issue.
- Some combos need monitoring: Fish oil + blood thinners isn’t banned, but your doctor should know.
- A few are “don’t mix” situations: St. John’s Wort + antidepressants, potassium + ACE inhibitors, red yeast rice + statins.
- 2026 trend alert: Adaptogens like ashwagandha can affect thyroid meds — don’t add them blindly.
- “Natural” doesn’t mean safe: Melatonin adds sedation, CoQ10 affects warfarin, milk thistle drops blood sugar.
- Your pharmacist is underused: They can spot interactions your doctor might miss.
This guide covers the 17 most common supplement interactions, with severity ratings and what to actually do about each one. Updated February 2026.
Here’s something that surprises most people: about 57% of American adults take at least one supplement, and over half take prescription medications — but almost nobody checks whether they play nicely together. Or they try to Google it and get conflicting answers from sites that haven’t been updated since 2019.[1]
With the rise of potent adaptogens (ashwagandha, rhodiola) and high-dose nootropics in 2026, interaction risks have shifted from simple vitamins to complex herbal stacks. This is exactly why we built PharmaGuide — an AI trained on clinical interaction data to give you clear, personalized answers.
The good news? Most common supplement interactions aren’t dangerous. They’re just… annoying. Your calcium blocks your thyroid med. Your magnesium makes your antibiotic less effective. You’re spending money on something that isn’t absorbing properly.
But some interactions matter more. Fish oil can amplify blood thinners. St. John’s Wort can mess with antidepressants, birth control, and HIV medications. Vitamin K can make warfarin unpredictable.
This guide covers the interactions I see most often — the ones that trip up real people taking real supplements. For each one, I’ll tell you: what happens, how serious it is, and what to do about it. If you want to check your own stack, you can see how our interaction checker works.
Let’s start with the basics.

Why Supplements and Medications Interact
Interactions happen for a few predictable reasons. Once you understand the patterns, you can often guess which supplements need spacing — even without looking it up.
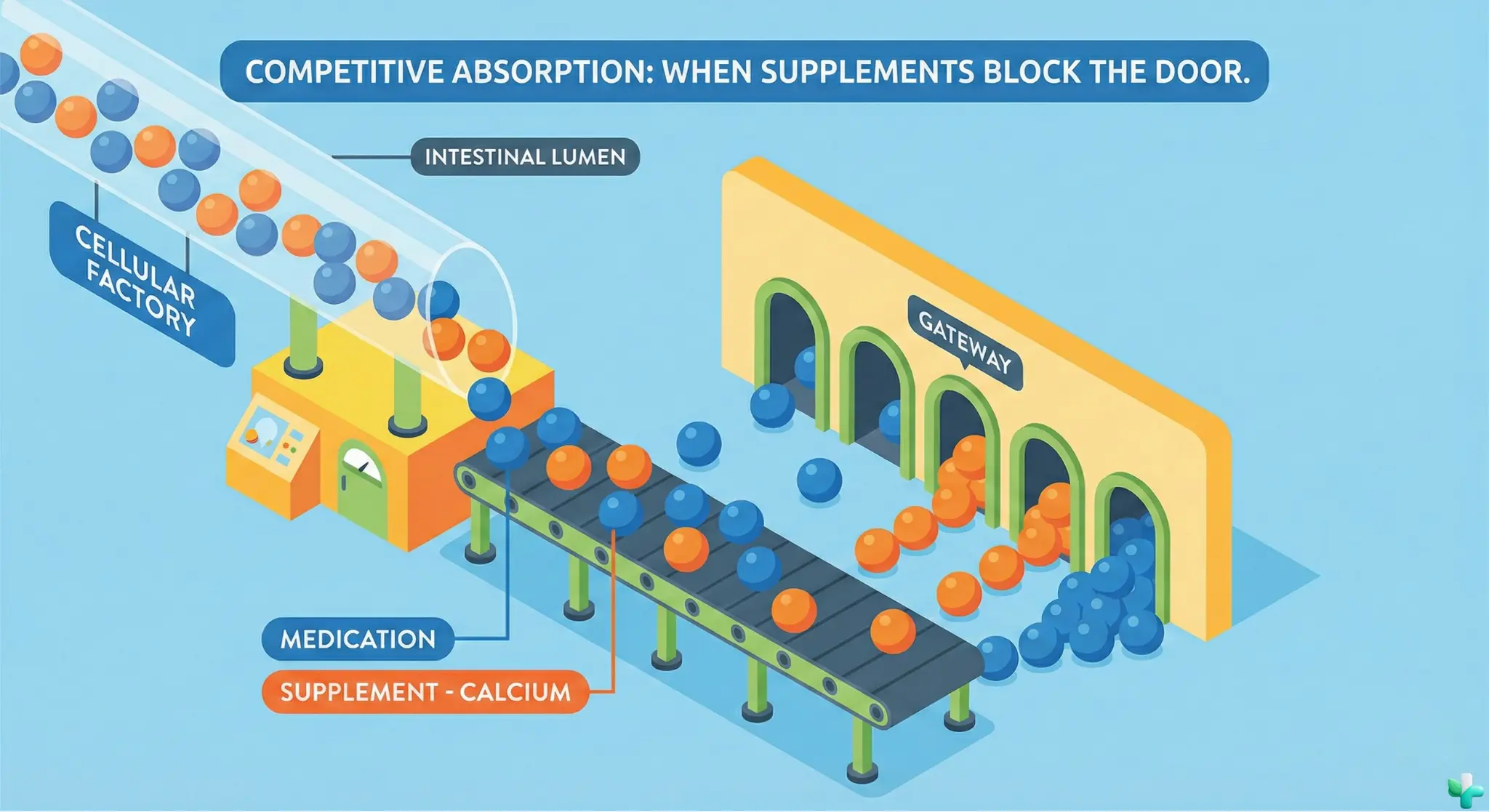
Pattern 1: Absorption blocking. Minerals like calcium, magnesium, iron, and zinc can physically bind to certain medications in your gut, forming a clump that neither can absorb properly. This is why thyroid meds, antibiotics, and osteoporosis drugs have strict “take on an empty stomach” rules.
Pattern 2: Same effect, stacked. If a supplement does something similar to your medication, the effects can add up. Fish oil thins blood mildly. So does aspirin. So does warfarin. Stack all three and bleeding risk goes up — not because any one is dangerous, but because they’re all pushing in the same direction.
Pattern 3: Enzyme competition. Your liver uses enzymes (especially one called CYP3A4) to break down many medications. Some supplements — St. John’s Wort is the worst offender — can speed up or slow down these enzymes, changing how fast your body clears a drug.[2]
Severity Levels in This Guide
I’ll rate each interaction using four levels:
- High — Avoid this combination or requires close medical supervision
- Moderate — Manageable with timing or monitoring, but tell your doctor
- Low — Minor effect, usually fixed with simple spacing
- Generally Safe — Theoretical concern but rarely a problem in practice
These ratings reflect consensus from clinical references and pharmacist guidance — see our methodology for rating interactions.
Now let’s get into the specific interactions.
17 Common Supplement Interactions (And What to Do)
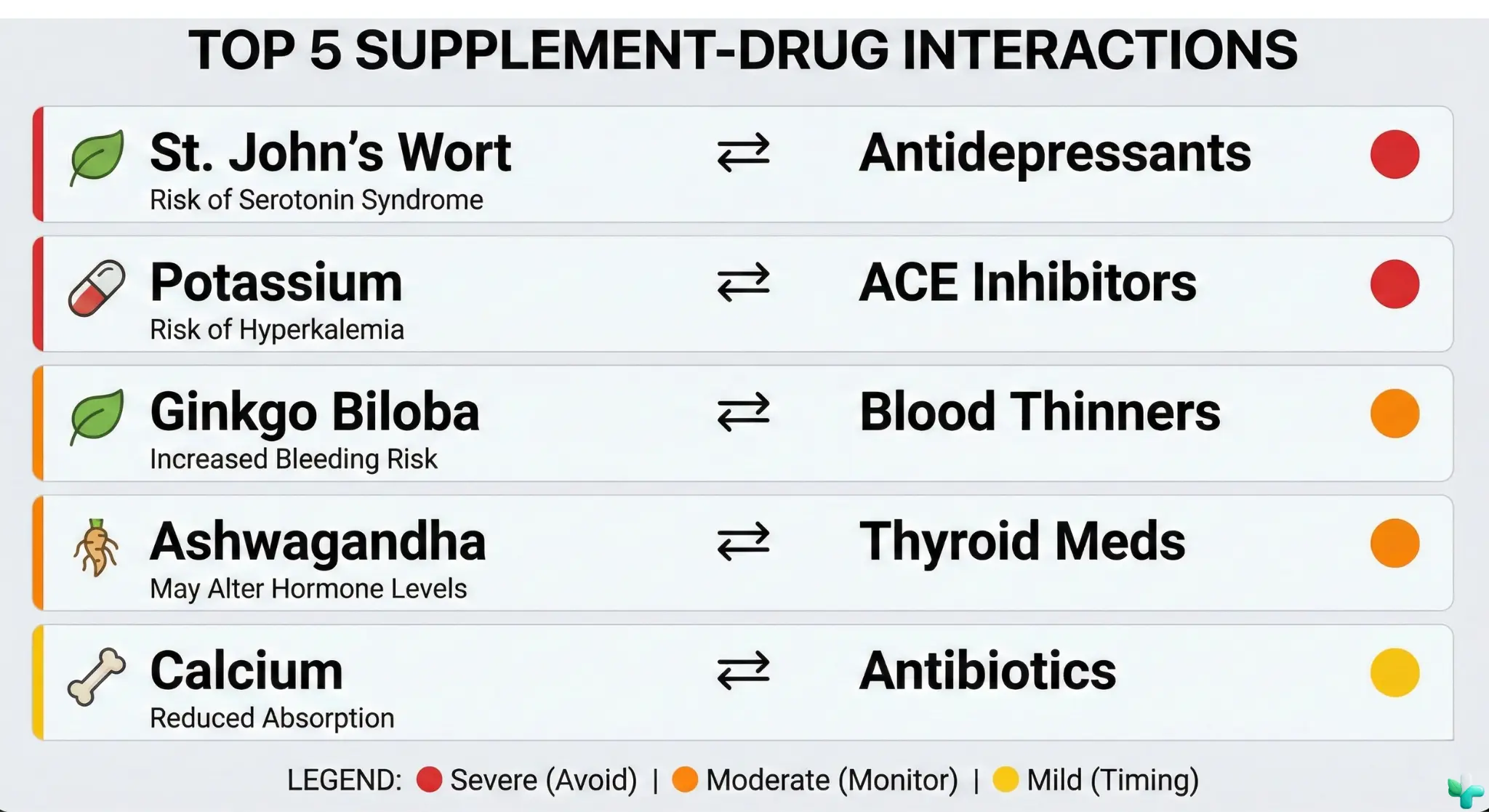
1. Calcium + Thyroid Medication
Moderate
What happens: Calcium binds to levothyroxine (Synthroid, Levoxyl, Tirosint) in your stomach, reducing absorption by up to 20-25%. You take your thyroid med, but less of it actually reaches your bloodstream.[3]
What to do: Take levothyroxine first thing in the morning on an empty stomach. Wait at least 4 hours before calcium supplements, calcium-fortified foods, or antacids containing calcium.
Real-world note: This is one of the most common reasons people have “unstable” thyroid levels. If your TSH keeps bouncing around, ask your pharmacist about timing.
2. Magnesium + Antibiotics
Moderate
What happens: Magnesium binds to fluoroquinolone antibiotics (ciprofloxacin/Cipro, levofloxacin/Levaquin) and tetracyclines (doxycycline, minocycline), and can dramatically reduce absorption — in some cases by more than 50%.[4]
What to do: Separate magnesium supplements from these antibiotics by at least 4-6 hours. Take the antibiotic first if you have to choose. The antibiotic course is temporary — being flexible with your magnesium timing for a week won’t hurt you.
Real-world note: This also applies to calcium, iron, and zinc. If you’re on a short antibiotic course, consider pausing mineral supplements entirely until you’re done.
3. Fish Oil (+ Garlic, Vitamin E) + Blood Thinners
Moderate
What happens: Fish oil has mild antiplatelet effects. Combined with warfarin (Coumadin), apixaban (Eliquis), rivaroxaban (Xarelto), or even daily aspirin, it can increase bleeding risk — especially at higher doses.[5]
Also in this category: Garlic supplements (especially aged garlic extract) and high-dose vitamin E (above 400 IU/day) have similar antiplatelet effects. If you’re on blood thinners, all three should be on your “tell your doctor” list.[15]
What to do: Tell your doctor you’re taking fish oil, garlic, or vitamin E. They may want to monitor your INR more closely (if on warfarin) or adjust your dose. Most people can continue these at modest doses, but they shouldn’t be secrets.
Real-world note: Tell your surgeon in advance if you take fish oil, garlic supplements, or high-dose vitamin E — they may ask you to stop 1–2 weeks before some procedures.
4. St. John’s Wort + Antidepressants (and Many Other Medications)
High
What happens: St. John’s Wort increases serotonin. So do SSRIs like sertraline (Zoloft), fluoxetine (Prozac), and escitalopram (Lexapro). Together, they can cause serotonin syndrome — a potentially serious condition with symptoms like agitation, rapid heartbeat, high blood pressure, and confusion.[6]
What to do: Don’t combine them. If you’re on an antidepressant and want to try St. John’s Wort, talk to your prescriber about transitioning — never overlap.
St. John’s Wort: The “High-Interaction” Supplement
St. John’s Wort speeds up drug metabolism via CYP3A4 enzymes, reducing the effectiveness of many medications to potentially dangerous levels. The NCCIH documents clinically significant interactions with:[14]
- Immunosuppressants (cyclosporine, tacrolimus) — organ rejection risk in transplant patients
- HIV medications (indinavir, other antiretrovirals) — viral rebound, treatment failure
- Oral contraceptives — breakthrough bleeding, unintended pregnancy
- Warfarin (Coumadin) — reduced anticoagulation, clot risk
- Digoxin — reduced heart medication effectiveness
- Benzodiazepines — reduced sedative effect
- Paxlovid (nirmatrelvir/ritonavir) — reduced COVID-19 antiviral effectiveness
If you take any prescription medication, treat St. John’s Wort as “ask your pharmacist first.”
Too much to remember? You don’t need to memorize this list. PharmaGuide AI automatically scans your specific supplements against your meds to find hidden conflicts — with timing recommendations built in.
5. Vitamin K + Warfarin
Moderate
What happens: Warfarin works by blocking vitamin K’s role in blood clotting. If your vitamin K intake swings wildly — a big salad one day, none the next — your INR becomes unpredictable, increasing clotting or bleeding risk.[7]
What to do: You don’t have to avoid vitamin K — you need to be consistent. Eat roughly the same amount of leafy greens each week. If you take a vitamin K supplement (including some multivitamins), keep the dose steady and tell your anticoagulation clinic.
Real-world note: This doesn’t apply to newer blood thinners like Eliquis or Xarelto — they work differently and aren’t affected by vitamin K.
6. Iron + Thyroid Medication
Moderate
What happens: Just like calcium, iron binds to levothyroxine and reduces absorption. Many people take both — especially women with heavy periods and hypothyroidism.[3]
What to do: Separate by at least 4 hours. Morning thyroid med, evening iron (or vice versa) is a common approach. Iron is better absorbed on an empty stomach but can be taken with food if it upsets your stomach.
7. Ginkgo Biloba + Blood Thinners
Moderate
What happens: Ginkgo has mild antiplatelet effects — similar to aspirin. Stacked with warfarin, aspirin, or other blood thinners, bleeding risk increases. Case reports include unusual bruising and prolonged bleeding after minor cuts.[8]
What to do: If you’re on anticoagulants, skip ginkgo or get your doctor’s okay. Stop ginkgo at least 2 weeks before any surgery.
8. Calcium + Bisphosphonates (Osteoporosis Meds)
Moderate
What happens: Alendronate (Fosamax), risedronate (Actonel), and similar osteoporosis drugs have notoriously strict absorption requirements. Calcium, coffee, food — basically anything — dramatically reduces how much gets absorbed.[9]
What to do: Take your bisphosphonate first thing in the morning with plain water. Stay upright for 30 minutes. Wait at least 30-60 minutes before calcium, food, or coffee. Yes, it’s annoying. Yes, it matters.
9. Zinc + Copper (Supplement-Supplement)
Low
What happens: High-dose zinc (over 40mg/day for extended periods) can block copper absorption, potentially causing copper deficiency over time. Symptoms include anemia and neurological issues — but this takes months of high-dose zinc to develop.[1]
What to do: If you’re taking zinc long-term at higher doses (for acne, immune support, etc.), look for a supplement that includes a small amount of copper, or take them at different times. Short-term zinc for a cold? Don’t worry about it.
10. Licorice (Glycyrrhizin) + Digoxin / Diuretics / Blood Pressure Meds
High (in digoxin or potassium-depleting diuretic users)
What happens: Real licorice (not artificially flavored candy) contains glycyrrhizin, which causes your kidneys to retain sodium and water while excreting potassium. This leads to hypokalemia (low potassium) — a dangerous state that increases arrhythmia risk and can be fatal in people on certain heart medications.[21]
Who’s most at risk:
- Digoxin (Lanoxin) users: Low potassium makes digoxin toxicity more likely — potentially causing dangerous heart rhythms
- Diuretic users (thiazides, loop diuretics): These also lower potassium, so the effect stacks — potentially to critical levels
- Blood pressure medication users: Licorice’s sodium-retaining effect can counteract antihypertensives
What to do: If you take digoxin, diuretics, or BP medications, avoid real licorice (including licorice root tea, supplements, and European-style licorice candy). Most American licorice candy is flavored with anise and doesn’t contain glycyrrhizin — but check the label. The Merck Manual recommends complete avoidance for these patient groups.[21]
Real-world note: This interaction trips up people who think licorice tea or “natural” licorice supplements are harmless. Glycyrrhizin effects can persist for weeks after stopping — it’s not a quick fix.
11. Biotin + Lab Tests (Bonus: Not a Drug Interaction, But Critical)
Moderate
What happens: High-dose biotin (often marketed for hair, skin, and nails — typically 5,000-10,000 mcg) can interfere with certain lab tests that use biotin-based technology. This includes some thyroid panels (TSH, T3, T4) and cardiac troponin tests (used to diagnose heart attacks). The result? False readings that can lead to misdiagnosis or missed diagnoses.[11]
What to do: If you’re taking high-dose biotin and have labs scheduled — especially thyroid or cardiac — stop biotin 48-72 hours before your blood draw. Tell your doctor and the lab that you’ve been taking biotin. This doesn’t affect all tests, but thyroid and troponin are the big ones.
Real-world note: The FDA issued a safety communication about this in 2017 after reports of missed heart attack diagnoses. It’s not about biotin being dangerous — it’s about biotin fooling the test.
12. Ashwagandha + Thyroid Medication
Moderate
What happens: Ashwagandha is an adaptogen that has exploded in popularity for stress and testosterone support. But it can naturally stimulate thyroid hormone production. If you’re already taking levothyroxine (Synthroid, Levoxyl) for hypothyroidism, ashwagandha can push you from “normal” into “hyperthyroid” territory — causing anxiety, heat intolerance, rapid heartbeat, and weight loss.[12]
What to do: You don’t necessarily need to stop ashwagandha, but you must tell your endocrinologist before starting it. They may want to check your TSH levels more frequently or adjust your levothyroxine dose. Don’t just add ashwagandha because a podcast told you to.
Real-world note: Ashwagandha also has mild sedative effects, so be cautious combining it with sleep medications or benzodiazepines (like Xanax or Ativan) — the drowsiness can stack.
13. Potassium Supplements + ACE Inhibitors / Spironolactone
High
What happens: This one is genuinely dangerous. ACE inhibitors (lisinopril, enalapril, ramipril) and spironolactone (a diuretic often used for blood pressure, acne, or hormone therapy) both raise potassium levels. Add a potassium supplement on top, and you can develop hyperkalemia — dangerously high potassium that can cause serious heart rhythm disturbances, sometimes without clear early symptoms.[13]
What to do: If you’re on an ACE inhibitor or spironolactone, do not take potassium supplements unless your doctor specifically prescribes them and monitors your levels. This includes “lite salt” (potassium chloride) and some electrolyte drinks. If you need more potassium, get it from food — bananas and potatoes are safer because the dose is lower and more gradual.
Real-world note: This interaction is a silent killer because hyperkalemia often has no symptoms until it’s an emergency. It’s one of the strongest arguments for checking your stack before adding anything new.
14. Melatonin + Sedatives / Blood Pressure Meds / Diabetes Meds
Moderate (can be High in older adults or polypharmacy)
What happens: Melatonin is one of the most-used supplements — but it’s not as “harmless” as people assume. The main practical risk is additive sedation with benzodiazepines (Xanax, Ativan, Valium), Z-drugs (Ambien, Lunesta), and other CNS depressants, increasing fall risk especially in older adults. Melatonin may also worsen blood pressure control in people already on BP medications, and may affect glucose tolerance in some people with diabetes.[16]
What to do: If you’re on sedatives, blood pressure medications, or diabetes medications, tell your doctor before adding melatonin. Start with the lowest dose (0.5–1 mg) rather than the 5–10 mg doses commonly sold. Monitor for excess drowsiness, dizziness, or blood sugar changes.
Real-world note: The “melatonin + sedative” combination is particularly risky in older adults because of fall risk. A 2 AM bathroom trip while double-sedated is how hip fractures happen.
15. CoQ10 + Warfarin
Moderate
What happens: This one is the opposite of fish oil and ginkgo. CoQ10 (ubiquinone) is structurally similar to vitamin K, which means it may reduce warfarin’s blood-thinning effect — potentially leading to clots, not bleeding. Your INR may drop unexpectedly if you start CoQ10.[17]
What to do: If you’re on warfarin and want to take CoQ10 for heart health or statin-related muscle symptoms, tell your anticoagulation clinic. They may need to check your INR more frequently when you start or stop CoQ10. This interaction is manageable — it’s not “never take it” — but it requires monitoring.
Real-world note: Many people on statins also take CoQ10 for muscle symptoms, and many statin patients are also on blood thinners. This is a common real-world overlap that often gets missed.
16. Milk Thistle + Diabetes Medications
Moderate
What happens: Milk thistle (silymarin) is commonly used for “liver support” — but it may also lower blood sugar. If you’re already on glucose-lowering medications like metformin, sulfonylureas (glipizide, glyburide), or insulin, milk thistle can add to the effect and cause hypoglycemia (low blood sugar).[18]
What to do: If you have diabetes and want to try milk thistle, monitor your blood sugar more closely when you start. Watch for symptoms of hypoglycemia: shakiness, sweating, confusion, rapid heartbeat. You may need to adjust your diabetes medication dose — work with your prescriber, don’t just wing it.
Real-world note: People often take milk thistle because they’re worried about their liver (sometimes due to statin use). If you’re also diabetic, this “protective” supplement could cause unexpected lows.
17. Red Yeast Rice + Statins
High
What happens: Red yeast rice contains monacolin K, which is chemically identical to lovastatin (Mevacor). That means red yeast rice is essentially a hidden statin. If you’re already taking a prescription statin like atorvastatin (Lipitor) or simvastatin (Zocor), you’re doubling your statin exposure — increasing risk of muscle damage (myopathy), liver problems, and rhabdomyolysis.[19]
What to do: Don’t take red yeast rice if you’re on a statin. If you want to use red yeast rice instead of a statin (some people try this for “natural” cholesterol control), that’s a conversation with your doctor — not a DIY switch. And be aware that red yeast rice products vary wildly in monacolin K content, so dose control is poor.[20]
Real-world note: Some people stop their statin because of muscle pain, then start red yeast rice thinking it’s “natural” — and get the same muscle pain because it’s the same drug. If you had statin side effects, red yeast rice is likely to cause them too.
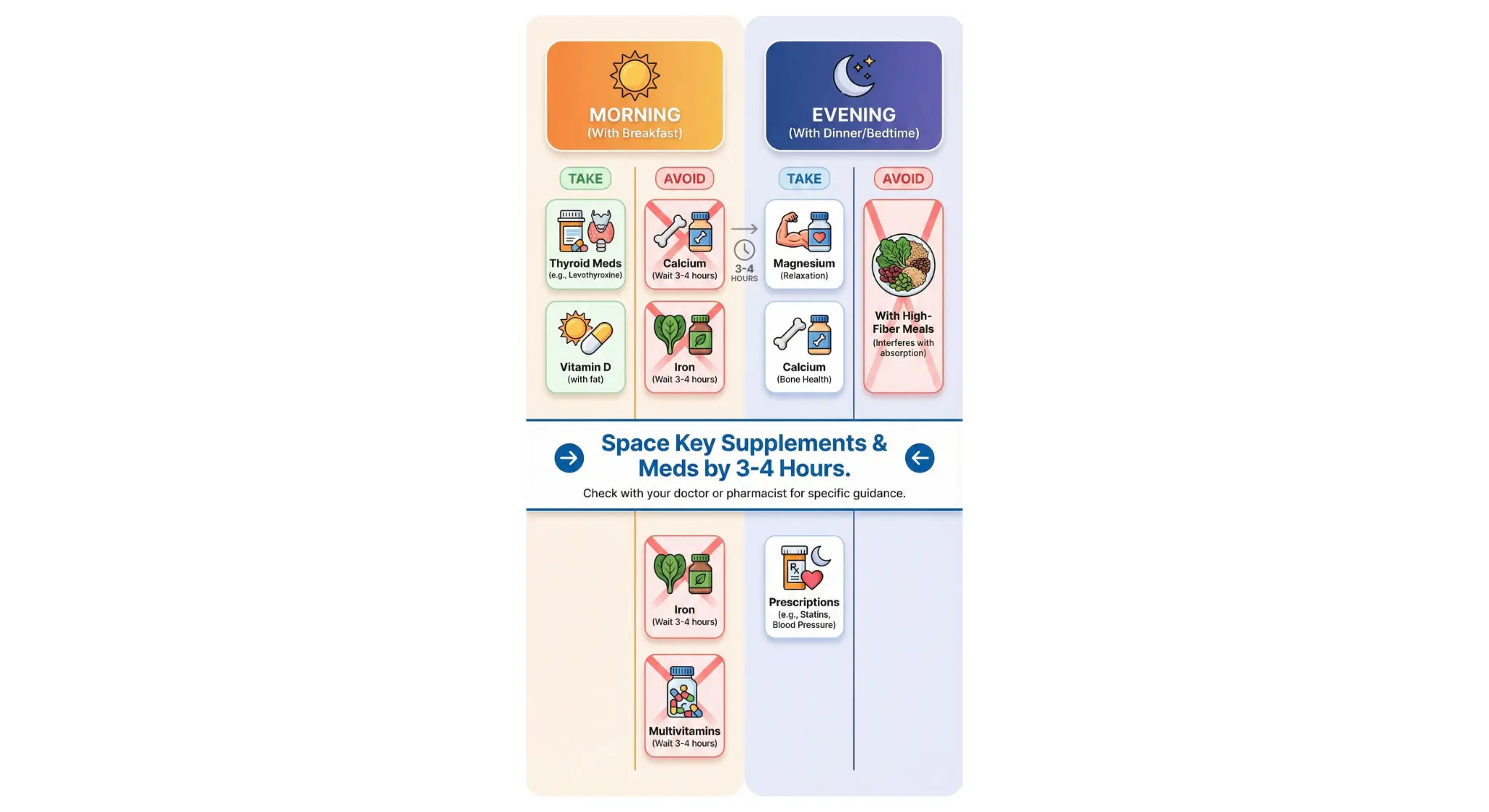
How to Manage Supplement Timing (Without Going Crazy)
If you’re taking multiple supplements and medications, timing can feel overwhelming. Here’s a practical framework:
| Time of Day | What to Take | Notes |
|---|---|---|
| First thing (empty stomach) | Thyroid medication, bisphosphonates Wait 30-60 min before food, coffee, or supplements | These are the most absorption-sensitive |
| With breakfast | Most vitamins, fish oil Fat-soluble vitamins (A, D, E, K) absorb better with food | Start your day’s supplements here |
| Midday (if needed) | Second dose of vitamin C, B vitamins Water-soluble vitamins don’t stick around — splitting helps | Optional for most people |
| Evening / with dinner | Magnesium, calcium, iron Minerals that might interact with morning meds | 4+ hour gap from thyroid/antibiotics |
When to Talk to Your Pharmacist
Your pharmacist can see your complete medication list and often catches interactions that doctors miss. Bring your supplement bottles to your next prescription pickup and ask: “Can you check if any of these interact with my medications?”
This is free, takes 5 minutes, and could save you from a problem you didn’t know you had.
Red Flags That Suggest an Interaction Problem
- Your medication “stopped working” — especially thyroid meds or antibiotics
- Unusual bruising or bleeding — if you’re on blood thinners + fish oil/ginkgo
- Your lab values keep swinging — TSH, INR, or other monitored levels
- New side effects after starting a supplement — especially mood changes, heart racing, or GI issues
If any of these sound familiar, don’t just stop everything — talk to your prescriber about what to adjust.
The Bottom Line
Most common supplement interactions are manageable — they just require some awareness and timing. The big takeaways:
Key Takeaways
- Minerals (calcium, magnesium, iron, zinc) can block absorption of thyroid meds and antibiotics — space by 4+ hours
- Antiplatelet supplements (fish oil, ginkgo, garlic, vitamin E) stack with prescription anticoagulants — tell your doctor
- St. John’s Wort interacts with antidepressants, birth control, HIV meds, transplant drugs, and many others — treat as “ask first”
- Potassium supplements + ACE inhibitors can cause dangerous hyperkalemia — don’t combine without monitoring
- Licorice (glycyrrhizin) causes potassium loss and can be dangerous with digoxin, diuretics, or BP meds
- Melatonin adds sedation and may affect BP/blood sugar in some people — not as harmless as assumed
- CoQ10 can reduce warfarin effectiveness (opposite of fish oil) — monitor INR
- Milk thistle may lower blood sugar — monitor if diabetic
- Red yeast rice IS a statin (contains lovastatin) — don’t stack with prescription statins
- High-dose biotin can interfere with thyroid and cardiac lab tests — stop 48-72 hours before blood draws
- Your pharmacist is your best free resource for checking interactions
For more guides on specific combinations, check out more safety and interaction guides.
Common Questions
What’s the most dangerous supplement interaction?
St. John’s Wort with SSRIs (antidepressants) is one of the most serious because it can cause serotonin syndrome — a potentially life-threatening condition. St. John’s Wort also interacts with birth control, HIV medications, and blood thinners. If you take prescription medications, St. John’s Wort should be a “talk to your doctor first” supplement.
How far apart should I take supplements from medications?
For most absorption-based interactions (calcium + thyroid meds, magnesium + antibiotics), 4 hours is the standard recommendation. For bisphosphonates (Fosamax, etc.), 30-60 minutes minimum before any food or supplements. When in doubt, morning medication and evening supplements is a safe default.
Can I take fish oil if I’m on blood thinners?
Usually yes, but your doctor should know. Fish oil has mild blood-thinning effects that can add to prescription anticoagulants. At modest doses (1-2g/day), it’s often fine with monitoring. At higher doses or before surgery, it may need to be stopped. The key is transparency — don’t hide it from your healthcare team.
Do I need to avoid vitamin K if I’m on warfarin?
No — you need to be consistent, not avoidant. Warfarin’s effectiveness depends on your vitamin K intake being stable. Eat roughly the same amount of leafy greens each week, and don’t suddenly start or stop vitamin K supplements. Your INR will be much more stable if your diet is predictable.
Will my doctor know about supplement interactions?
Not always. Many doctors have limited training on supplement interactions, and supplements aren’t always in their prescribing software. Pharmacists often catch interactions that doctors miss because they see your complete medication list. Bring your supplement bottles to the pharmacy and ask for a quick review.
Are “natural” supplements safer than medications?
Not necessarily. “Natural” doesn’t mean “no interactions.” St. John’s Wort is a plant, and it’s one of the most interaction-prone supplements out there. Ginkgo, grapefruit, and licorice root all have significant drug interactions despite being natural. Always check — don’t assume safety based on the source.
Should I stop my supplements before surgery?
Some supplements — including fish oil, garlic, ginkgo, vitamin E, and St. John’s Wort — may need to be stopped 1–2 weeks before certain surgical procedures due to bleeding or medication interaction risk. Always tell your surgeon about every supplement you take so they can advise you on timing.
Sources & References (21 citations)
- National Institutes of Health, Office of Dietary Supplements. “Dietary Supplements: What You Need to Know.” View Source
- U.S. Food and Drug Administration. “Drug Interactions: What You Should Know.” View Source
- Liwanpo L, Hershman JM. “Conditions and drugs interfering with thyroxine absorption.” Best Pract Res Clin Endocrinol Metab. 2009;23(6):781-792. PMID: 19942153
- Neuhofel AL, et al. “Lack of bioequivalence of ciprofloxacin when administered with calcium-fortified orange juice.” J Clin Pharmacol. 2002;42(4):461-466. PMID: 11936572
- Bays HE. “Safety considerations with omega-3 fatty acid therapy.” Am J Cardiol. 2007;99(6A):35C-43C. PMID: 17368277
- Izzo AA, Ernst E. “Interactions between herbal medicines and prescribed drugs: an updated systematic review.” Drugs. 2009;69(13):1777-1798. PMID: 19719333
- Booth SL, Centurelli MA. “Vitamin K: a practical guide to the dietary management of patients on warfarin.” Nutr Rev. 1999;57(9):288-296. PMID: 10568340
- Kellermann AJ, Kloft C. “Is there a risk of bleeding associated with standardized Ginkgo biloba extract therapy?” Pharmacotherapy. 2011;31(5):490-502. PMID: 21923430
- Porras AG, et al. “Effect of food on the bioavailability of alendronate.” Clinical Pharmacology & Therapeutics. 1999;66(6):608–613. PMID: 10630309
- Bailey DG, et al. “Grapefruit-medication interactions: forbidden fruit or avoidable consequences?” CMAJ. 2013;185(4):309-316. PMID: 23184849
- U.S. Food and Drug Administration. “The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication.” 2017. View Source
- Sharma AK, et al. “Efficacy and Safety of Ashwagandha Root Extract in Subclinical Hypothyroid Patients.” J Altern Complement Med. 2018;24(3):243-248. PMID: 28829155
- Palmer BF. “Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system.” N Engl J Med. 2004;351(6):585-592. PMID: 15295051
- National Center for Complementary and Integrative Health (NCCIH). “St. John’s Wort and Depression: In Depth.” View Source
- Asher GN, Corbett AH, Hawke RL. “Common Herbal Dietary Supplement-Drug Interactions.” Am Fam Physician. 2017;96(2):101-107. PMID: 28762712
- Mayo Clinic. “Melatonin: Overview, Uses, Side Effects, Precautions, Interactions.” View Source
- Drugs.com. “Coenzyme Q10 and Warfarin Drug Interaction.” Professional Interaction Monograph. View Source
- Mayo Clinic. “Milk Thistle: Overview, Uses, Side Effects, Precautions, Interactions.” View Source
- Mayo Clinic. “Red Yeast Rice: Overview, Uses, Side Effects, Precautions, Interactions.” View Source
- National Center for Complementary and Integrative Health (NCCIH). “Red Yeast Rice: What You Need to Know.” View Source
- Merck Manual Professional Edition. “Licorice: Dietary Supplements.” View Source
Check Your Supplement Stack
Knowing about common supplement interactions is the first step. PharmaGuide’s AI Pharmacist can check your specific combination of supplements and medications — with timing recommendations tailored to your routine.
Join the Waitlist →